Overview & Profile
We are developing a unique series of selective thyroid hormone receptor beta (TRβ) agonists for metabolic disorders. Our lead clinical program’s drug candidate, VK2809, is a novel, orally available small molecule thyroid hormone receptor agonist that possesses selectivity for liver tissue, as well as the beta receptor subtype, suggesting promise for the treatment of metabolic disorders, including non-alcoholic steatohepatitis (NASH).
About
In November 2019, we initiated the VOYAGE study, a Phase 2b clinical trial designed to assess the efficacy, safety, and tolerability of VK2809 in patients with biopsy-confirmed NASH and fibrosis. The primary endpoint of the study, the reduction in liver fat content at 12 weeks, was successfully achieved in May 2023, when the company announced that VOYAGE had demonstrated statistically significant reductions in liver fat from baseline to Week 12 in patients receiving VK2809 as compared to placebo. Adverse events (AEs), including GI-related AEs, were similar among VK2809-treated patients vs. placebo, so overall tolerability remains encouraging. Secondary objectives include the evaluation of histologic changes assessed by hepatic biopsy after 52 weeks of treatment. Viking announced the successful achievement of these secondary objectives in June 2024.
The Phase 2b VOYAGE study follows a previous successful Phase 2a trial for the treatment of non-alcoholic fatty liver disease (NAFLD) and elevated low-density lipoprotein cholesterol (LDL-C), where patients who received VK2809 demonstrated statistically significant reductions in LDL-C and liver fat content compared with patients who received placebo. VK2809 has been evaluated in eight completed clinical studies, which enrolled more than 300 subjects. No serious adverse events, or SAEs, have been observed in subjects receiving VK2809 in these completed studies. In addition, the compound has been evaluated in chronic toxicity studies of up to 12 months in duration.
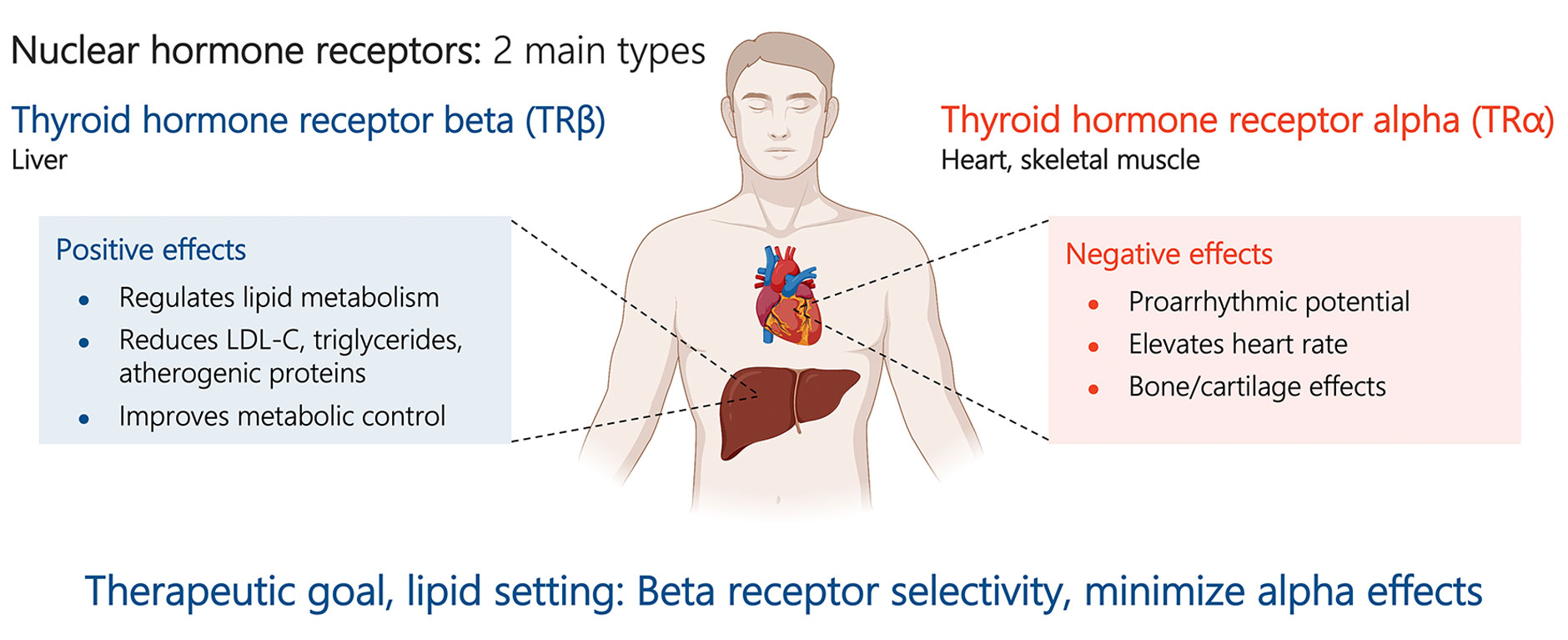
Thyroid hormone receptors are found in various tissues throughout the body. TRß is the major receptor isoform expressed in the liver and thyroid hormone receptor alpha, or TRα, is the major isoform expressed in the heart. The liver-targeting properties of our TRβ agonists are designed to reduce or eliminate the deleterious effects of extra-hepatic thyroid receptor activation. In particular, high tissue and TRβ selectivity may lead to reduced activity at the TRα receptor, which can be associated with increased respiration and cardiac tissue hypertrophy. Selective activation of the TRß receptor in liver tissue is believed to favorably affect cholesterol and lipoprotein levels via multiple mechanisms, including increasing the expression of low-density lipoprotein receptors and increasing mitochondrial fatty acid oxidation. These characteristics in turn lead to reductions of LDL-C, plasma and liver triglycerides.
Various animal models have shown that our molecules, as a result of their unique profiles, may have reduced cardiovascular effects versus thyroid hormone and other thyromimetics. As a result of these characteristics, we believe our selective TRß agonists are capable of eliciting a unique lipid lowering profile without eliciting unwanted effects on the heart and thyroid hormone axis.
Clinical Data: Phase 2b Study
Primary Endpoints
The Phase 2b VOYAGE study successfully achieved its primary endpoint, with patients receiving VK2809 experiencing statistically significant reductions in liver fat content from baseline to Week 12 as compared with placebo. The median relative change from baseline in liver fat as assessed by MRI-PDFF ranged from 38% to 55% for patients receiving VK2809. Importantly, up to 85% of patients receiving VK2809 experienced at least a 30% relative reduction in liver fat content, a level of reduction that is associated with greater likelihood of histologic response in NASH. Additionally, and consistent with prior studies, patients receiving VK2809 demonstrated statistically significant placebo-adjusted reductions in LDL-C ranging from 11% to 20%, as well as statistically significant reductions in triglycerides and atherogenic proteins such as apolipoprotein B (ApoB), lipoprotein (a) [Lp(a)], and apolipoprotein C-III (ApoC-III). Reductions in these plasma lipids improve a patient’s overall cardiometabolic profile and may reduce the risk of cardiovascular-related events. VK2809 demonstrated encouraging safety and tolerability in this study. The majority (94%) of treatment-related AEs among patients receiving VK2809 were reported as mild or moderate. Discontinuations due to AEs were low and balanced among placebo and treatment arms. One treatment-related SAE was reported in a patient receiving VK2809. A patient with a history of psychiatric disorders reported a worsening of their symptoms. As in prior studies, VK2809 demonstrated excellent gastrointestinal (GI) tolerability in this study. Rates of nausea, diarrhea, stool frequency, and vomiting were similar among VK2809-treated patients compared to placebo.
Secondary Endpoints
The Phase 2b VOYAGE study also successfully achieved its secondary endpoints evaluating histologic changes assessed by hepatic biopsy after 52 weeks of treatment with VK2809:
On the secondary endpoint of NASH resolution with no worsening of fibrosis, VK2809-treated patients demonstrated NASH resolution ranging from 63% to 75%, compared with 29% for placebo (p<0.05 for each VK2809 treatment group). Across the combined VK2809 treatment groups, 69% achieved NASH resolution (p<0.0001 vs. placebo). Resolution of NASH was defined as a non-alcoholic fatty liver disease activity score (NAS) of 0 or 1 for inflammation and 0 for ballooning.
On the secondary endpoint evaluating improvement in fibrosis with no worsening of NASH, VK2809-treated patients demonstrated improvement in fibrosis ranging from 44% to 57%, compared with 34% for placebo (p<0.05 for the 5 mg and 10 mg QOD cohorts). Across the combined VK2809 treatment groups, 51% achieved improvement in fibrosis with no worsening of NASH (p=0.03 vs. placebo). Improvement in fibrosis without worsening of NASH was defined as a ≥1-stage improvement in fibrosis and no increase in NAS for ballooning, inflammation, or steatosis.
On the secondary endpoint evaluating the proportion of patients experiencing both resolution of NASH and improvement in fibrosis, VK2809-treated patients demonstrated improvement ranging from 40% to 50%, compared with 20% for placebo (p<0.05 for the 5 mg and 10 mg QOD cohorts). Across the combined VK2809 treatment groups, 44% achieved this endpoint (p=0.003 vs. placebo).
Clinical Data: Phase 2a Study
The previous 12-week, Phase 2a clinical trial of VK2809 in patients with NAFLD and elevated LDL-C successfully achieved its primary endpoint. Patients receiving VK2809 demonstrated statistically significant reductions in LDL-C of 20% or more, compared with placebo-treated patients. In addition, VK2809-treated patients demonstrated statistically significant improvements in other lipids, including atherogenic proteins apolipoprotein B and lipoprotein (a). In addition, the trial’s secondary endpoint was achieved, since patients receiving VK2809 experienced reductions in liver fat content of 54%-60%, as assessed by MRI-PDFF, which were statistically significant relative to placebo, after 12 weeks of treatment. In terms of safety and tolerability, no SAEs were reported among patients receiving VK2809 or placebo. Mean alanine aminotransferase, or ALT, levels among patients receiving VK2809 were reduced relative to those of patients receiving placebo. Among patients with elevated baseline ALT levels, those receiving VK2809 also demonstrated reduction relative to placebo. There were no clinically or numerically meaningful differences in direct bilirubin, indirect bilirubin, alkaline phosphatase or international normalized ratio (INR) between patients treated with VK2809 or placebo. In addition, no meaningful changes to the thyroid hormone axis were observed among VK2809-treated patients compared with placebo-treated patients.
Clinical Data: Phase 1 Studies
VK2809 has also been evaluated in seven Phase 1 clinical trials. The initial Phase 1 (safety, tolerability, and pharmacokinetic study of VK2809) was followed by a 14-day Phase 1b, multiple-ascending dose clinical trial in 56 patients with mild hypercholesterolemia. In this Phase 1b study, patients who received VK2809 demonstrated significant reductions in LDL-C, triglycerides and atherogenic proteins.1,2 VK2809 was shown to be safe and well-tolerated in this study. VK2809 was evaluated in five additional Phase 1 trials, evaluating the pharmacokinetics, pharmacodynamics, potential drug-drug interaction of VK2809 when co-administered with a statin, alternative dosing regimens and hepatic impairment, respectively.
Preclinical Data
In a rodent model of diet-induced NASH, VK2809 has demonstrated potent reductions in plasma and liver lipids, as well as improvements in liver fibrosis. VK2809-treated rodents also demonstrated improvement in genes associated with lipid metabolism and suppression of genes associated with fibrogenic signaling.
In animal models of hypercholesterolemia, or high levels of cholesterol in the blood, VK2809 demonstrated promising reductions in plasma cholesterol with minimal effects on the thyroid hormone axis at doses effective for cholesterol reduction.3,4
Thyroid Hormone Receptor Overview
Hypercholesterolemia, Fatty Liver Disease and NASH
The desirable cholesterol levels are less than 200 mg/dL for total cholesterol, and less than 100 mg/dL for LDL-C (“bad” cholesterol).5,6,7 In the US, the number of adults age 20 or older that have total cholesterol levels ≥ 200 mg/dL is nearly 94 million8,9, and those that have LDL-C levels ≥ 130 mg/dL is nearly 70 million.9
The global prevalence of NAFLD is approximately 25%.10 In the US, it was estimated that 64 million individuals have NAFLD,11 which corresponds to a prevalence of approximately 20%. NAFLD can lead to NASH, a severe form of liver diseases which involves inflammation and cell damage. NASH is a growing epidemic and is quickly becoming a leading cause of cirrhosis and liver failure. It is estimated that the overall prevalence of NASH is between 1.5% and 6.45% of the population.10
References:
- Lian B, Hanley R, Schoenfeld S. A Phase 1 Randomized, Double-Blind, Placebo-Controlled, Multiple Ascending Dose Study to Evaluate Safety, Tolerability and Pharmacokinetics of the Liver-Selective TR-Beta Agonist VK2809 (MB07811) in Hypercholesterolemic Subjects. Poster presented at the 2016 Meeting of the American College of Cardiology (link).
- Schoenfeld SL, Lian B, Hanley R, Homer K. Reduction of Atherogenic Lipoprotein (a) and Apolipoprotein B in Humans with the Selective Thyroid Receptor Beta Agonist VK2809. Poster presented at the American Heart Association 2016 Scientific Sessions (link).
- Fujitaki JM, Cable EE, Ito BR, Zhang BH, et al. Preclinical Pharmacokinetics of a HepDirect Prodrug of a Novel Phosphonate-Containing Thyroid Hormone Receptor Agonist. Drug Metab Dispos. 2008; 36(11):2393-2403 (link).
- Erion MD, Cable EE, Ito BR, Jiang H, et al. Targeting Thyroid Hormone Receptor-Beta Agonists to the Liver Reduces Cholesterol and Triglycerides and Improves the Therapeutic Index. Proc Natl Acad Sci U S A. 2007;104(39):15490-15495 (link).
- CDC: Getting Your Cholesterol Checked (link)
- Grundy SM, Stone NJ, Bailey AL, Beam C, et al. 2018 ACC/AHA/AACVPR/AAPA/ ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082–e1143 (link).
- National Institutes of Health (National Heart, Lung and Blood Institute). National Cholesterol Education Program: Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III), Final Report. September 2002 (link).
- CDC: High Cholesterol Facts (link)
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2021 Update: A report from the American Heart Association. Circulation. 2021;143:e254–e743 (link).
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, et al. Global Epidemiology of Nonalcoholic Fatty Liver Disease–Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology. 2016;64:73-84 (link).
- Younossi ZM, Blissett D, Blissett R, Henry L, et al. The Economic and Clinical Burden of Nonalcoholic Fatty Liver Disease in the United States and Europe. Hepatology. 2016;64:1577-1586 (link).